
Ortho-K for Myopia Control in Kids
Ortho-K for Myopia Control in Kids
 If your child’s prescription is climbing every year, Ortho-K is one of the most studied tools we have to slow that progression. Custom contact lenses worn overnight reshape your child’s cornea while they sleep. Studies show roughly 50% slower progression in kids on Ortho-K compared to standard glasses or daytime contacts. Beyond the myopia control benefit, your child wakes up to a day that doesn’t include glasses or daytime contacts at all.
If your child’s prescription is climbing every year, Ortho-K is one of the most studied tools we have to slow that progression. Custom contact lenses worn overnight reshape your child’s cornea while they sleep. Studies show roughly 50% slower progression in kids on Ortho-K compared to standard glasses or daytime contacts. Beyond the myopia control benefit, your child wakes up to a day that doesn’t include glasses or daytime contacts at all.
If you’re still comparing all the myopia control options, our Myopia Management page walks through them side by side. If you want to know what Ortho-K is, how the corneal reshaping works, what it costs, and what the COVE process looks like, our main Ortho-K page covers all of that. This page is the deep dive on Ortho-K specifically as a myopia control treatment for kids.
Why Ortho-K has become a leading choice for childhood myopia
Two reasons families pick Ortho-K, and both are real.
The first is daytime convenience. Your child wakes up with clear vision, takes the lenses out, and goes through their day with no glasses and no daytime contacts. School, sports, swim practice, all of it.
The second reason, and the one that drives most of the consultations we do, is myopia control. Ortho-K has the largest body of peer-reviewed research for slowing childhood myopia of any treatment available. Studies have shown that overnight Ortho-K reduces the rate of axial elongation, the eye’s growth that drives worsening nearsightedness, by 36 to 56% on average compared to standard glasses [1, 2]. A 2023 review specifically of Euclid Emerald Ortho-K lenses (the design we use most often at COVE) analyzed 14 controlled studies and found a mean reduction in axial growth of 0.28 mm at two years [1].
One of our own patients came to us at age 8 with a prescription already at -6.00 diopters, which is well above what we typically see at that age. We started him on Ortho-K right away. He’s 14 now, seeing great, and his prescription has barely moved in six years.
In plain language: kids on Ortho-K end up with weaker prescriptions as adults than they would have without treatment. Our Myopia Management page explains why that matters for long-term eye health.
How we decide between Ortho-K and the other myopia control options
At your child’s exam we look at three things: how active they are, what their prescription looks like (especially astigmatism), and what kind of treatment experience your family is looking for. The right choice usually comes down to one of those three factors.
Ortho-K is usually the right pick when:
- Your child is very active in sports, especially water sports. Swimmers do well with Ortho-K because there are no daytime lenses to lose in the pool. Same logic applies to gymnasts, soccer players, wrestlers, and any sport where glasses or daytime contacts are a hassle or a hazard.
- Your child has mild to moderate myopia with relatively mild astigmatism. We say more about astigmatism in the candidacy section below.
- Your family prefers a treatment that’s done by the time the day starts. No drops to remember, no daytime lenses to insert before school.
MiSight 1-Day soft contact lenses tend to fit better when your child wants a more traditional contact lens experience or prefers a daytime lens to an overnight one.
Stellest spectacle lenses tend to work better for kids with higher astigmatism that limits Ortho-K results, kids who don’t want to wear contacts at all, or families who prefer the simplest treatment plan.
Low-dose atropine drops are an option for kids who can’t tolerate any contact lens, and we sometimes combine atropine with Ortho-K or MiSight for additional effect.
For a full side-by-side comparison of all four treatments, see our Myopia Management page. At your child’s exam we’ll walk through the options and recommend the one that fits.
Is my child a candidate for Ortho-K?
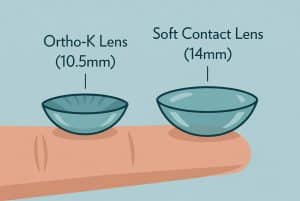
Ortho-K lenses are about 25% smaller in diameter than standard soft contact lenses (10.5mm vs 14mm).
Most kids who do well with Ortho-K share a few characteristics:
- They’re typically between 7 and 16 years old. Age 8 to 12 is the sweet spot for starting because that’s when myopia tends to progress fastest.
- Their nearsightedness falls in the range Ortho-K corrects best (roughly -0.75 to -6.00 diopters, sometimes higher with custom lens designs).
- Their astigmatism is manageable. Up to about 1.50 diopters is usually straightforward. Above that, achieving sharp daytime vision gets harder, but it’s not an automatic disqualification. What matters more is whether the astigmatism is corneal (caused by the shape of the front of the eye) or internal (caused by the lens inside the eye). Ortho-K reshapes the cornea, so it can correct corneal astigmatism. It cannot change internal astigmatism. We can’t tell which is which without a corneal topography scan, which is part of the evaluation we do at the exam.
- They’re mature enough to be a partner in their own care, with a parent’s help in the early weeks.
The only way to know for sure is the topography scan and a thorough exam. We do this as part of a regular comprehensive eye exam at COVE, not a separate consult, so there’s no extra appointment to book.
What a typical day with Ortho-K looks like
 Bedtime: your child puts the lenses in (most kids 8 and up can do this themselves after a couple weeks of practice; younger kids usually have a parent help). They go to sleep.
Bedtime: your child puts the lenses in (most kids 8 and up can do this themselves after a couple weeks of practice; younger kids usually have a parent help). They go to sleep.
Morning: they take the lenses out, clean them, put them in the case. That’s the entire daytime routine. No glasses to lose. No contacts to insert before school. No fog on the goggles at swim practice. No lens problems mid-game during soccer.
For active kids, that’s the whole appeal. The morning after their first night, they wake up and see clearly, and they go through their day the way a kid who never needed glasses would. After school, screen time, sleepovers, summer camp, all of it works without anything in their eyes.
Why families across Central Ohio choose COVE for kids’ Ortho-K
Dr. Amy Keller has 25+ years of pediatric optometry experience and has guided hundreds of myopic kids through their treatment journeys, from first prescription through stable adult outcomes. Dr. Matthew Karres has presented research on specialty contact lens design at international conferences and stays current with the latest in custom lens technology and topography-based fitting.
We use Euclid Emerald lenses for most of our pediatric Ortho-K patients because the design has the longest peer-reviewed research record of any Ortho-K lens (over 20 years on the market and used on more than two million eyes worldwide). For kids whose corneas need a more custom fit, we use WAVE NightLens, a fully bespoke lens designed from your child’s individual corneal topography rather than picked from a parameter set. We are one of very few practices in Ohio that fit WAVE lenses.
We also do the Ortho-K evaluation as part of a regular comprehensive eye exam, not as a separate consult or premium-fee visit. The topography scan and exam findings are part of what we do anyway, regardless of which treatment we end up recommending. Most insurance covers the comprehensive exam, and the candidacy discussion is part of the visit either way.
Frequently asked questions about Ortho-K for kids
How young can my child start Ortho-K?
Most kids start Ortho-K between ages 7 and 10. Age 8 to 12 is the sweet spot because myopia tends to progress fastest in that window, and most kids in that age range are mature enough to be partners in their own care with a parent’s help in the early weeks. We’ve fit children younger when there’s a clear clinical reason and the family is on board, and we’ve started kids as old as their late teens.
Will my child need Ortho-K forever?
We typically recommend staying on treatment until age 18 to 20. The honest answer is that it’s hard to know exactly when treatment is no longer needed because every kid is different, but by the late teens or very early 20s, the eye is usually done growing and myopia tends to stabilize. At that point your child can stop wearing the lenses and the cornea will revert to its natural shape over a couple of weeks. They’ll need glasses or contacts (or LASIK eventually) to correct whatever prescription they ended up with, but the goal of Ortho-K is to make sure that final prescription is as low as possible.
Can my child put the lenses in by themselves?
Most kids age 8 and up can learn to insert the lenses on their own within the first couple weeks of treatment. For younger kids, parents typically help for the first few months and then the child takes over. We coach the whole process at the dispensing visit and we’re available for questions any time after.
Can my child play sports and swim with Ortho-K?
Yes, that’s one of the biggest reasons parents choose it. Because the lenses come out in the morning, your child can play sports, swim (we still recommend goggles for chlorine protection), do gymnastics, wrestle, and live their normal life with no eyewear during the day. For swimmers especially, Ortho-K is often the safest choice because there are no daytime lenses to risk losing in the pool.
How is Ortho-K different from MiSight or atropine?
All three slow myopia progression. Ortho-K and MiSight are both contact lenses; Ortho-K is worn at night and reshapes the cornea while MiSight is a soft contact lens worn during the day. Atropine is an eye drop used at bedtime, and unlike the lens options it doesn’t correct the vision itself, so kids on atropine usually still wear glasses. We talk through all three at the exam and recommend the one that fits your child’s prescription, activity level, and your family’s preferences.
What about sleepovers and summer camp?
Lenses travel with your child. They go in the case at the host’s house or at camp the same way they go in at home. Most kids handle the routine without parental help by their second year on treatment. We do recommend bringing solution and a backup case in case anything gets misplaced.
My child has astigmatism. Can they still do Ortho-K?
Possibly. Up to about 1.50 diopters of astigmatism is usually straightforward. Higher than that, achieving great daytime vision becomes harder, though custom lens designs can extend the range. The other factor is whether the astigmatism is corneal (which Ortho-K can reshape) or internal (which it cannot). We use a topography scan at the exam to measure both. If your child has high or mostly internal astigmatism, Stellest spectacle lenses or another option may fit better.
Ready to find out if Ortho-K is right for your child?
At COVE, the Ortho-K evaluation is part of a regular comprehensive eye exam. There’s no separate consult to book and no extra fee to find out if your child is a candidate. We’ll do the topography scan, review the prescription history, walk through every option (Ortho-K, MiSight, Stellest, atropine), and tell you honestly which one we think fits best. Most insurance covers comprehensive exams, and the candidacy discussion is part of the visit either way.
Schedule your child’s comprehensive eye exam online or call us at (614) 933-0575.
References
[1] Bullimore MA, Mirsayafov DS, Khurai AR, et al. Efficacy of the Euclid orthokeratology lens in slowing axial elongation. Contact Lens & Anterior Eye. 2023.
[2] A 2023 multi-site analysis of childhood myopia management (the CAMP study). Treehouse Eyes.